The Chemo Question (and other stories)
It’s been a while since I posted, and it’s been an interesting and educational few weeks. When last we left the saga of Mary’s boobs, the tumor had been removed, at least one lymph node was involved, and the pathology revealed some lymphovascular invasion (that is, most of the cancer in the involved node had moved out of the node itself into the surrounding tissue). Thus began my education into current breast cancer thinking, which it turns out is a liminal miasma of studies, philosophies, competing predictor models, metaphysics, luck, gut instinct, and other stuff. I say liminal, because the science surrounding my kind of cancer straddles the historical divide between the recent past, when they threw chemo at everything, and the near future, when they will tailor the treatment to the tumor’s genome, because soon everyone will have genomes, even tumors.
Straddling the Liminal Space (in the Country of Africa—that part’s for Laura)
For example, the question of cutting. Because I had a lumpectomy instead of a mastectomy, doctors assumed I would have radiation eventually, so they didn’t find out there was cancer in one sentinel lymph node (sentinel means closest to the breast) until after the operation was over. Had they gotten those results when they were still in the thick of things, so to speak, they would have just removed the remaining nodes. But to go back in and remove them later, and then irradiate them, would have upped my chances of lymphedema to more than 50% (lymphedema is a permanent and unpleasant condition for which they make awful compression sleeves that cause consternation on breast cancer support sites). So many doctors argued first among themselves, and then with me, about whether to do a second surgery. What was the likelihood that cancer had spread to the other nodes?
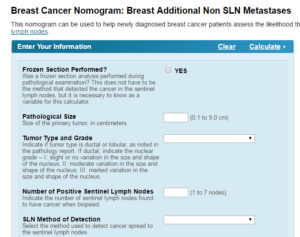
Luckily, the nation’s two leading cancer centers have online “nomograms” to help you guess. Sloan Kettering said I had a 12% chance of additional node involvement. MD Anderson said my chances were 67%. The data each nomogram asks you to input are very different, and obviously the results are too. They differ because each school considers different factors to be important when calculating your odds. Predictably the “tumor board” in Atlanta that debated my treatment went many rounds on this question of cutting out the nodes or not. One shining young radiation oncologist and breast enthusiast (he recognized the skilled hand of my plastic surgeon at once) spent an hour first telling me to have surgery and then telling me not to have it. The final decision was that, since I was likely to have chemo anyway, we would skip the surgery and let chemo and radiation chase down the putative stray cells as they cascaded headlong through my hapless blood stream.
But then came the debate about chemo—one that is still ongoing. Online predictors like Predict! (http://www.predict.nhs.uk/predict.html if you want to try it yourself), suggest that the benefit of chemo for someone like me is small but substantive, adding two percentage points to my five-year survival chances, and four percentage points to my ten-year survival chances. But the Predict! Tool (imagine pink letters and a breast-cancer ribbon in place of the “I”) isn’t tailored to the particular biology of one’s particular tumor. For this, you need to go to one of many obscenely expensive services that give you a genomic profile of your cancer. The best-researched of these is called the Oncotype DX, and here is where religion comes into play.
The Altar of the Onctype
The Oncotype test looks at 21 genomic thingies, plus it tells you just exactly how receptive your cancer is to estrogen, progesterone, and her2 proteins (don’t ask me what her2 proteins are). And for about $4000, it gives you a score and a graph. The score is between 1 and 100, and if your score is low, the thinking is that chemotherapy definitely will do more harm than good, and you have a low chance of your cancer returning. If your score is high, then chemotherapy is definitely for you, because without it your cancer has a higher chance of recurring. If your score is intermediate, then they have just thrown up their hands and billed your insurance. To add to the confusion, the Oncotype company thinks low is 1-18, while the studies out there validating it define low as 1-10. High, for the company, is 30 and above, while the large studies define high as over 25. The validity of high and low results have been fairly well established, but for some reason the researchers decided to sit on the intermediate results (11-25 or 19-30, depending) for another year or so, so no one really knows exactly what it means to have an intermediate score.

My score, as you might expect, is 19, which is either the lowest possible intermediate score, or right smack in the middle of intermediate, depending on whom you ask. If you look at the graph, 19 is right at the point where the line saying “chemo won’t help you a bit” crosses the line that says “chemo will be your savior.” The company says that with my lymph node involvement, my cancer has a 12% chance of recurring in the next five years, with chemo OR without chemo. It doesn’t predict longer down the road, when one’s odds of recurrence and other bad things inevitably go up. But while seeing your chances quantified is really not fun and makes you want to curl up in a ball forever, a 12% chance of doom isn’t as scary as it could be, especially since more effective hormone inhibitors exist now, improving the odds all the time.
Back to Competing Prediction Models
So which model do you go with when deciding to get chemo? For academics and “true believers” like the second oncologist I saw in Atlanta, you must love the Oncotype DX with all your soul and with all your might. “If you do chemo, it will be an emotional decision, not a rational one,” he said loftily. For my local oncologist and other doctors I’ve asked, relying on the Oncotype DX alone and not choosing chemo is just too risky, maybe because they’re uncertain about the data or maybe because not recommending chemo hangs them out to dry if someone gets a recurrence and says, “If only I’d had chemo!” After all, if you never know why cancer recurs, you will always think the one thing you didn’t do was the deciding thing. “It’s different out here in the world, where chemo is still the standard of care,” said one doctor. Chemo is what insurance companies recommend; in fact, with a positive lymph node like mine, they don’t even like to pay for the Oncotype DX test. (I’ll spare you the story of how long it took to pry my results from the cold dead fingers of the company, who was holding them hostage while it negotiated with BlueCross). “What about that lymph node?” asks another. The true believers say that the radiation will take care of the lymph node. “But are they sure?” demands yet another, pointing to the Predict! Model. “What if a tiny cancer cell has traveled somewhere else and is waiting to hatch somewhere else?” They point to the fact that the new chemotherapy drugs may work better (the Oncotype test predicts your odds using the old chemotherapy drugs). I located a study saying even the new chemotherapy drugs didn’t affect my cancer much. But that study only looked at the odds over three years, which may not be enough to tell anything. In other words, in ten more years, everyone is going to know a whole lot more about whether I should have chemo, but my cancer is happening now. And even though time feels circular and arbitrary, it is still linear where it hurts.
The reason the choice is important is that the new chemos have large odds (15% or more) of causing long-term-to-permanent loss of brain function, weight gain, and neuropathy. And maybe leukemia. These all sound unpleasant, but if you know me, you know that my brain function—especially verbal function—is really important to me. But is it so important that death would be preferable to losing it? I do not rightly know the answer. To me, this is such a classically literary dilemma that it feels unreal. It’s just the sort of metaphysical exploration of meaning that ought to be crowned with an epiphany and a denouement. And oncologists line up on either side of this divide, hurling insults at each other, while I struggle with the basic question of who I am and what I live for. I need to speak to the writer.
The Most Unkindest Cut
Meanwhile, the boobs remain impossibly perky and are healing at a good rate, but there’s still a one-centimeter hole I have to pack twice a day. Various packing solutions, including some weird little strips called “lodoform packing strips” that look like confetti, have taken turns being inserted in there to prevent something called tunneling; so far, all have been gross and yet inadequate, but they allow me to poke things into the hole while calling it the most unkindest cut of all, cackling with fevered desperation. Also, the boobs are still pretty swollen, so I have gained an education in compression bras and physical therapy. For boobs, PT involves letting a stranger in a labcoat stroke your lymph glands so lightly that you wouldn’t know she was there except that she bills your insurance.
MASS Confusion (PS the Puritans hated puns)
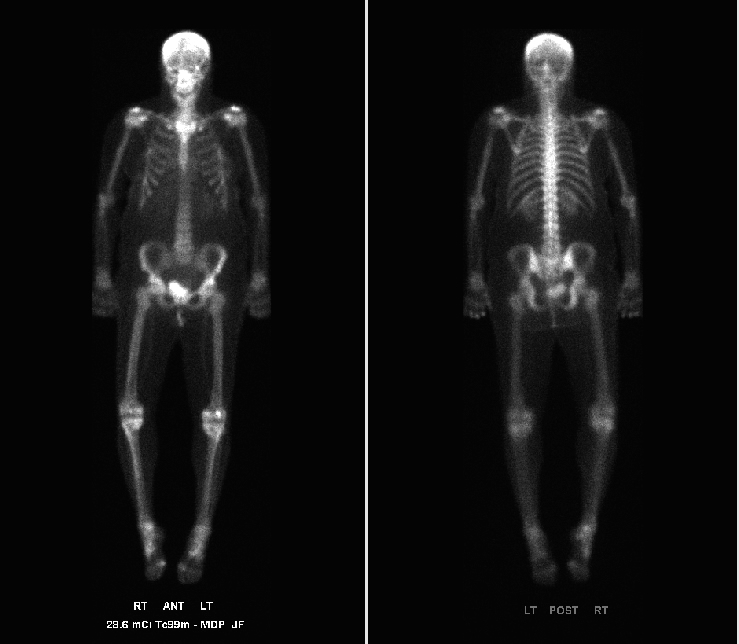
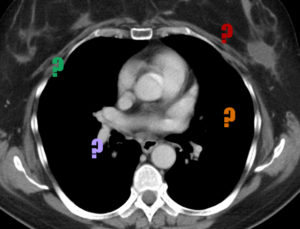
In the midst o f all this data, my ever-vigilant oncologist, a full-throated pragmatist, ordered a bunch of body scans just to make sure the cancer hadn’t spread already. These included a bone density scan (I have osteopenia, and I’m actually getting shorter!), a bone scan (the disk I obtained through the tender mercies of Carol the navigator says that the pictured skeleton is mine. I can’t prove it, but it has no cancer in it, so I’ll take it), and a CT scan of my guts. I admire the radiologists who have to read these things, because I have no idea what each organ is, since the photos show only large, undulating, undifferentiated constellations of chaos in which some of my Facebook friends think they see a dead squirrel, the hand of a vestigial twin, or the burgeoning fetus of Golem. Even the radiologist must finally have thrown up her hands and concluded formally that additional floating things had been detected and required further investigation. In other words, they could be masses, or blood vessels, or fatty intrusions, or hemangiomas, or spare change. In seconds, my oncologist was on the phone, ordering an MRI of my liver and a transvaginal ultrasound, just to be sure.
f all this data, my ever-vigilant oncologist, a full-throated pragmatist, ordered a bunch of body scans just to make sure the cancer hadn’t spread already. These included a bone density scan (I have osteopenia, and I’m actually getting shorter!), a bone scan (the disk I obtained through the tender mercies of Carol the navigator says that the pictured skeleton is mine. I can’t prove it, but it has no cancer in it, so I’ll take it), and a CT scan of my guts. I admire the radiologists who have to read these things, because I have no idea what each organ is, since the photos show only large, undulating, undifferentiated constellations of chaos in which some of my Facebook friends think they see a dead squirrel, the hand of a vestigial twin, or the burgeoning fetus of Golem. Even the radiologist must finally have thrown up her hands and concluded formally that additional floating things had been detected and required further investigation. In other words, they could be masses, or blood vessels, or fatty intrusions, or hemangiomas, or spare change. In seconds, my oncologist was on the phone, ordering an MRI of my liver and a transvaginal ultrasound, just to be sure.

The picture below accurately shows what it took to get me in that MRI machine, if you imagine a large bottle of ativan right beside it. As a side note, I would like to discuss my theories about the voices of machines, especially in doctor’s offices. Clearly, market research must have proven that women’s voices are more soothing, as the voices of machines in all of my doctor’s offices are female. “Going up,” says the elevator softly. “Please pay now,” lulls the Parking Validation machine. At any rate, the inventors of the MRI machine in Sylva added none of the frills (films of butterflies, soothing elevator music, cappuccino machine) to their long donut of doom. So it shouldn’t have surpised me that the MRI-machine voice is an angry, hoarse masculine cross between an obscene phone caller and a garbage disposal. “Breath in!” it growls, then “Hooooold your breath!” followed by a series of long guttural beeps that cease only when you’re allowed to breathe again—all while making 28% more than the voices of female machines.

The Transvaginal Ultrasound, which sounds like either a Seismic Phenomenon or a really scary ride at Dollywood, was called in to examine a four-centimeter mass in Ladytown, as my friend Catherine likes to call it. It is not all that reassuring to sit with your feet in stirrups while someone waves a wand around in Ladytown as gray blobs float about the screen and a doctor, two technicians, and a nurse try to figure out which if any of those blobs are your ovaries. Apparently, Ladytown has well and truly closed down for the season, so none of these tests were any more conclusive than the CT scan or the MRI. Therefore, next week I am getting the second surgery of my life, a hysterectomy, and my dog sitters and chief Goon Kaleb will be pressed back into service. Also, my splendid sister-in-law Peggy is coming to look after things, so I hope she’s not too horrified by the stench of my abode.
Almost done….
Meanwhile, I’m prepared to finish up summer school next week, and then I will sit down and write better thank you cards to all of you who donated (and the funds were badly needed and helped so much!), or sent cards, or offered to help in a hundred other ways. But just in case my life falls short of my intentions, please know how much it has meant to me. Cancer tells you a lot about your friends, and for every friend you counted on who is tongue-tied or just absent, there are several you didn’t know you had who reach out with both hands. But I will tell you what I wish I had known when my friends needed help—they don’t need advice, or food, or even rides as much as they need people to just sit with them and watch television, or pet dogs, or win ten whole cents at the casino, so they can remember what normal feels like and not confront the abyss in awful solitude. As I have said before, I’m grateful, even when I just can’t talk about it. Especially then.
8 thoughts on “The Chemo Question (and other stories)”
Love you and have no idea what I’ll need to do.
But, I have cleaned up the rental house of my darling Jessy twice after she had crashed with mental illness.
So, I’m guessing we will be just fine, just not too many sleepovers, or I will fail to breathe, …permently.
If and when I get some kind of screwed up cancer and need someone to hassle my docs and read my scans, YOU ARE IT, THE ONE, THE ONLY ONE.
I’ve got kids, and grand kids and friends and neighbors, even fine doctors, but your blog is a real education. It’s going to take me 12-24 hours to begin to digest.
I’m here in St. L dining on my gourmet meal, prepared, as Betty would have in the day, by me. On my back porch, listening to classical music on my wireless speakers. I am SO cool.
This is after seeing a great new opera: Shalimar, The Clown.
Without the Adams to keep up with, I would be such a small town clod.
Now, I have to do dishes, laundry, organize my office and draft dog sitting instructions, pack for culture in Chicago, and laid back fine food and arts and, last but not least Mary, in NC.
Lots of grammatical mistakes, but you get the drift?
So…it would just kill them to say, “We don’t really know?” That’s not something twenty-first century people are allowed to do, and doing it would lay twenty-first century doctors open to malpractice suits? Honest to God.
In unrelated news, I think you should gather these together into a book when it’s over. Few blogs of any kind are quite so clear about everything strange and wrong with this process, even, or especially, for the largely-absent, and this is a book which, assuming cancer’s coming for all of us sooner or later, I’d like to read during the throes.
Yes, to what Catherine says, both things.
Hi Mary, I tried to leave a comment a couple of hours back but I guess it didn’t take. Thinking of you and hope to have you over to visit soon.
The thesis of my brilliant but lost post was that you should indeed make a book of this blog. The writing is not only crystal clear but totally engaging. My first take that didn’t take said this so much better. Alas. Now I’m in nap mode and can’t remember any of it.
The one thing you shouldn’t worry about is the brain cells. You have so many of them that I don’t believe you would miss 15% at all. After all, we only use about 5% of our brain cells so if you do the math (which I’m not), you would still be about 50% ahead of everyone else.
Let me know if the casino is on the list again. I haven’t been for a long time.
Good grief, Mary. I’ve been out of touch. No news on the blog or Fb as best I can tell. Don’t know what to say or ask, hesitating to sound more out of touch. ….. Okay, that’s all I can say about that.
Love&Peace, Marsha Lee
Comments are closed.